


Deformities and Heterometries of the Lower Limbs
Deformities and differences in length between the lower limbs can result from various causes, and modern orthopedic surgery offers effective correction.
WHAT THEY ARE
Deformities and heterometries (length differences) in the lower limbs are anomalies, either congenital or acquired, affecting the normal structure and mechanical configuration of the lower limbs. Deformities can be classified into functional forms, caused by joint contractures leading to an apparent length difference or alteration of the mechanical axis, and structural forms, resulting from bone anomalies at any level of the lower limbs or pelvis. Heterometries may be congenital, associated with isolated congenital orthopedic diseases, or part of complex syndromes. Acquired heterometries can develop due to traumas, infections, tumors, or other factors.
CAUSES
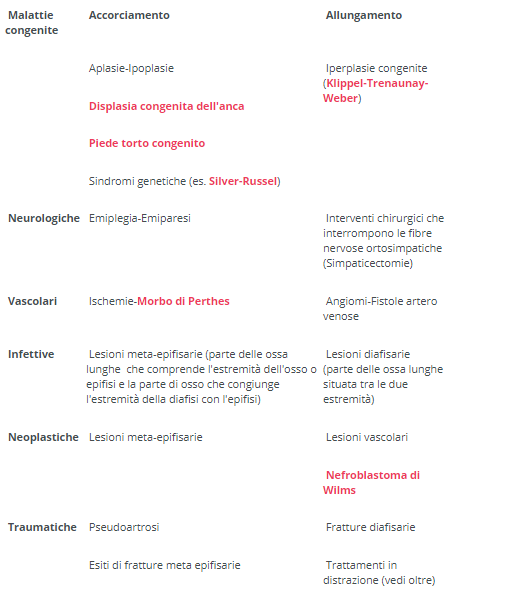
Congenital diseases causing lower limb heterometries are numerous, although in some cases, where no associated anomaly or apparent cause is detected, they may be idiopathic. The natural history of heterometries depends on the underlying disease. In congenital forms, deterioration is usually constant, and predicting the final length difference between limbs at the end of growth, aided by specialized software developed in recent years, is not difficult. Acquired forms exhibit extreme variability depending on the age of onset and severity. Diseases causing limb asymmetry can lead to shortening or lengthening of the affected limb. The table provides some examples.
DIAGNOSIS
Diagnosis primarily relies on clinical history and a thorough orthopedic examination. Precise determination of lower limb deformity or heterometry involves X-rays of the lower limbs under load—meaning with the patient standing—capturing front and side views, including the pelvis and ankles. Measurements include femur and tibia length, tracing the mechanical axes of the entire limb and individual bone segments, while also considering foot and hip anatomy. X-rays should be taken with compensatory elevation of the shorter limb.
TREATMENT
Deformities of the lower limbs should be treated, especially if they result from deficient or absent development of lower limb skeletal parts (congenital short femur, deficient or absent development of the tibia or fibula). If these deformities are idiopathic, lacking an apparent cause, they should be observed and potentially treated only in severe cases before the end of pubertal development. During this period, the growth plates of long bones, located at the metaphysis where the epiphysis and diaphysis meet, are active. After pubertal development, these growth plates fuse, and bones can no longer grow in length.
Surgical techniques like temporary hemiepiphysiodesis, also known as "controlled growth techniques," are employed. This technique temporarily halts bone growth on the inner or outer side, depending on the case. A U-shaped metal device, with parallel arms inserted into the growth plate, halts growth. The opposite part of the growth plate, with remaining growth, progressively corrects the deformity. The device is removed approximately one to two years after the intervention.
Length differences of 1 cm or less may not have immediate clinical relevance, often being observed and improving spontaneously towards the end of puberty. Length differences between 1 cm and 2 cm require careful observation, orthotic treatment (insoles with elevation and customized footwear) to decrease pelvic obliquity. In some cases, surgical treatment may be necessary. Length differences exceeding 2 cm typically require corrective surgical treatment.
The choice of surgical treatment for pediatric limb length discrepancies depends on the patient's age and the severity of the clinical picture. Surgical treatments considered include temporary or definitive hemiepiphysiodesis of the longer skeletal segment and lengthening of affected skeletal segments. Different methods, such as uniaxial external fixation, circular external fixation, hybrid external fixation (combination of axial and circular), external fixation with endomedullary nails, and motorized or magnetic telescopic endomedullary nails, can be used for pediatric limb lengthening.
Patients usually have a hospital stay of approximately 5-7 days. During this time, parents and the patient are educated about the lengthening process and daily care of wire tracts and screws that fix the external fixator to the limb. The patient cannot bear weight on the affected limb during the distraction (lengthening) phase but can gradually do so during the consolidation phase. Radiographic checks are performed weekly during the distraction phase and monthly during the consolidation phase. The fixator is removed when the lengthened skeletal segment shows evident bone restructuring on X-ray, in a Day Surgery setting. After fixator removal, patients may use a cast, brace, or walk without assistance.
written by: Pier Francesco Costici, Osvaldo Palmacci - Orthopedics Operational Unit in collaboration with Bambino Gesù Institute for Health
original article from ospedalebambinogesù.it