


Obstetric paralysis
Injuries to the nerves of the arms, forearms, and hands that, in most cases, can heal with simple early rehabilitation
WHAT IT IS
Obstetric injuries occur during childbirth, with the most severe being obstetric paralysis. Fractures of the clavicle (more common), shoulder dislocations, and epiphyseal separations of the humerus (rarer) are less severe. The use of cesarean section in challenging situations has reduced the frequency of these injuries. Traumatic maneuvers during childbirth can lead to neurological deficits in the newborn's arms, forearms, and hands, resulting from brachial plexus injuries—nerves that provide innervation to parts of the chest, shoulder, arm, and hand.
CAUSES
Factors favoring obstetric injuries include fetal macrosomia (birth weight over 4 kilograms) and difficult childbirth (dystocic). Dystocic childbirth occurs when natural delivery is challenging and requires intervention, such as forceps, vacuum extraction, or cesarean section. It can be due to difficulties in uterine contraction, issues with the dilation of the birth canal, pelvic shape hindering fetal exit, or fetal presentation anomalies, like breech presentation. In most cases, damage results from stretching of nerve fibers, rarely from tearing or complete rupture of one or more nerve roots.
HOW THEY MANIFEST
Three types of obstetric paralysis exist based on the affected nerve roots:
- Upper type (more common) caused by the injury of the fifth and sixth nerve roots, corresponding to cervical vertebrae C5-C6.
- Lower type (rarer) resulting from injury to the seventh and eighth nerve roots, corresponding to cervical vertebrae C7-C8, and the first dorsal nerve root, corresponding to dorsal vertebra D1.
- Total paralysis (very rare) caused by the injury of all nerve roots.
The newborn presents with the upper limb inert, extended along the trunk, and unresponsive to stimuli. In upper-type obstetric paralysis (Erb-Duchenne paralysis), the deficit primarily affects the shoulder and arm, appearing immobile with the elbow extended (adducted) and the arm and forearm rotated inward (internal rotation), causing the wrist to flex, the palm facing upward, and the back of the hand downward. Hand and wrist movements are preserved. In lower-type paralysis (Dejerine-Klumpke paralysis), the deficit mainly affects the hand. Flexing the wrist and fingers is challenging, and spreading the fingers like a fan (finger abduction) is difficult, while shoulder movements are preserved. Total paralysis combines symptoms from upper and lower types.
CAN THE DAMAGE BE RECOVERED?
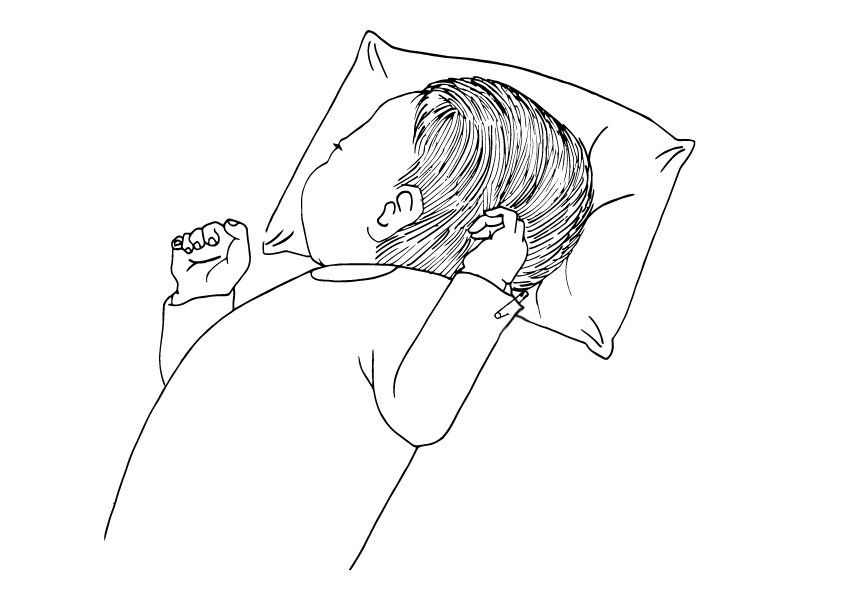
The recovery capacity varies based on the severity of the damage and the promptness of rehabilitative treatment, aiming to prevent joint deformities caused by persistent joint misalignments. Rehabilitation treatment should be immediate and daily, with better results achieved in upper-type paralysis. In the initial phase of upper-type obstetric paralysis, securing the newborn's upper limb to the bed pillow with a safety pin while resting in a supine position is useful. In severe cases of complete paralysis, surgical intervention is necessary to restore nerve trunk continuity within 4-8 months of birth. Untreated cases with prolonged duration result in a fixed flexed position of the arm and forearm. In these instances, muscle-tendon transposition surgeries are performed to compensate for deficient muscles. Rarer interventions involve bone procedures (humerus osteotomy) to externally rotate the arm.
written by: Pier Francesco Costici, Rosa Russo - Orthopedics Operating Unit
Illustrations by: Sara Suraci
In collaboration with: Bambino Gesù Institute for Health
Original article from: ospedalebambinogesù.it